Another week of headlines.
Millions
'wrongly attending' A&E. GP access
needs to improve. GPs could do more to
ease the burden on hospitals.
'Winter
is coming.'
So what
would happen if a practice opened the doors and allowed walk in access to its
patients for urgent conditions? No triage. No need to ring. Partners and nurse practitioners working as a team, average wait 30
minutes. The ability to phone if you
want to speak to someone.
The practice
We have a
large practice, across 4 sites, looking after over 27,000 patients. 14 partners, 3 nurse practitioners. Separate entrances and waiting rooms for the
urgent care service, based at the main site with 15,500 patients. We have just started a walk in service at one
of the branch surgeries this summer. We
have tried most systems over the years including telephone triage and
traditional on call models. There is no
additional contract for the service, it’s simply our model for our
patients.
The main
site is a few hundred yards from A&E.
There are areas of significant deprivation and high levels of chronic
disease, obesity and substance misuse including alcohol.
We have
partners with a high level of training and experience in a number of areas
including dermatology, orthopaedics, palliative care, substance misuse,
diabetes, ophthalmology and ENT.
The effect on the practice staff
The
service (known as LUCS – Larwood Urgent Care Service)
has been extremely popular. Routine surgeries are no longer overbooked and
receptionists now have no frustration finding appointments for patients wanting
to be seen urgently.
Staff
work extremely hard, and are proud of the service they help deliver.
Attendance levels
We opened
the service in November 2010 - at the start of a flu epidemic. We coped well with up to 140 contacts per
session that winter. As the service has
become established we have more stable numbers attending, less inappropriate
use and numbers have dropped slightly from 24,000 per year in 2010/11 and
11/12.
We are
able to predict attendance numbers and adjust staffing levels with higher
numbers attending on Monday, Tuesday and Fridays.
Patient
satisfaction levels are high, and we have seen and diagnosed a significant
amount of serious illnesses in the walk in service. Patients are asked their main problem as they attend to ensure
they do not have symptoms of a myocardial infarction or a stroke.
A&E attendances
The practice
is situated next to A&E and has a high level of morbidity and
deprivation. A&E attendance is
therefore higher than most other practices in the CCG with more rural
locations. A&E attendance overall has
reduced slightly, but less than we expected with a difference of 2-3%. We have seen an
increase in complex conditions in A&E and a reduction in minor illness
attendances requiring no investigations.
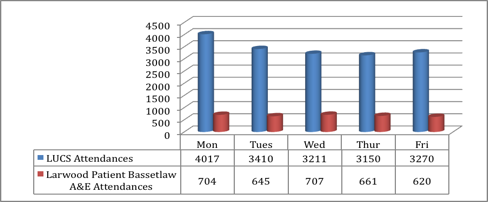 |
| 2012 Attendances By Day (in-hours) |
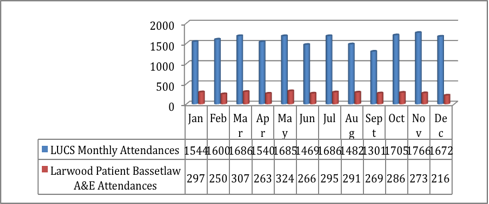 |
2012 Attendances by Month (in-hours)
|
 |
| Add caption |
Pressure on appointments
Routine
surgeries now have no extras, and visits seem to have reduced due to the
ability to be seen quickly at the surgery.
There is still a pressure on appointments and we continue to work on
this. We see a lot of patients, do
extended hours and have a large team of highly trained nursing staff. The service has improved the efficiency of
the practice and for a large urban practice the ability to separate acute and
planned care has undoubtedly been beneficial.
Wasted appointments
Despite
enabling online booking and texting reminders to patients before appointments
we had just under 10,000 appointments wasted last year due to DNAs. We are working with the patient group and
local media in an attempt to reduce this.
Conclusions
There are
many reasons why the walk-in service is better for the staff and our
patients. Reducing A&E attendance
was not a key driver in an area where inequalities are significant and
comorbidities common. Reducing
inappropriate A&E attendance was a driver, and we have had some success
with this.
Patients
attend A&E ‘inappropriately’ for many reasons.
Primary care access may be one, but deprivation, family culture, free
prescriptions and distance from A&E are key factors. We know that the ‘frequent attenders’ at A&E have mainly
alcohol or mental health problems, and it is essential that practices and CCGs
ensure services are commissioned to deal with these problems in an appropriate
setting.
There is
little evidence that we can prevent inappropriate A&E attendance through
education. We should focus on making
A&E safe, focus on staffing and pathways, and look to integrate services
(including primary care) where possible.
Blaming
GPs for not doing enough, or patients for attending, is not the answer.


